Researchers at the University of Pretoria (UP) have shown that a low-cost, easy-to-use screening device can detect foetal growth restriction in pregnant women, which, if not diagnosed, can lead to stillbirth, neonatal death or suboptimal childhood growth.
The work was done at UP’s Research Centre for Maternal, Fetal, Newborn and Child Health Care Strategies and published in peer-reviewed journal PLoS ONE.
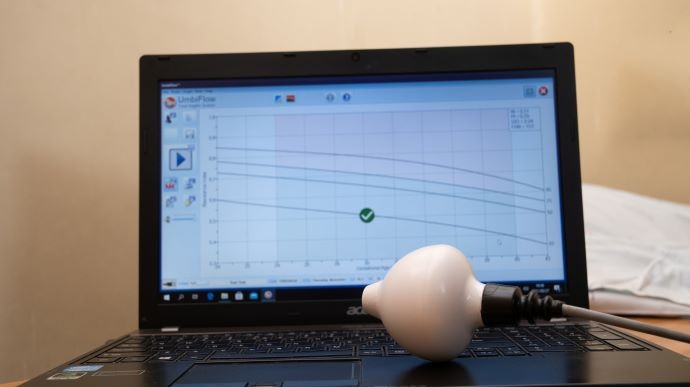
Dr Helen Mulol of the research centre and co-author of the study explains, "The UmbiflowTM is a portable, continuous-wave Doppler ultrasound device that was developed in South Africa and costs about one-tenth of a conventional ultrasound device. All healthcare workers, including nurses, can be trained relatively quickly to operate it. The device can be connected to a computer, tablet or smartphone and a printer can be attached to print out results".
Healthcare workers would use the UmbiflowTM to find the wave pattern of the umbilical artery which indicates the blood flow between the baby and the placenta.
From this wave pattern, a parameter called the resistance index (RI) can be calculated. The result of the RI, according to the gestational age of the baby, is plotted on a graph, with the next clinical management steps then being determined according to a “traffic light” system. According to risk categorisation, an RI value in the red or yellow region of the graph is classified as an “abnormal Doppler” and the mother is referred to an obstetrician or doctor for further investigation. An RI value in the green area is classified as a “normal Doppler”; this means the mother can continue antenatal follow-up visits at a local clinic.
The Doppler result is important because it is a measure of placental function – the rate of blood flow from the placenta to the foetus. Dr Mulol says foetal growth restriction can be defined as failure of the foetus to reach its genetic growth potential. “It does not mean that all growth-restricted babies are small,” she says. “It also does not mean that all small babies are growth restricted; some are just constitutionally small. Foetal growth restriction means the foetus is not growing as well as it should be in utero, which is exactly the group of babies that can be identified by the Doppler.”
Professor Ute Feucht – Director of the Research Centre for Maternal, Fetal, Newborn and Child Health Care Strategies, and lead author of the study – explains the implications: “The foetus is not receiving enough nutrition and oxygen in utero and therefore does not grow optimally. If this is not picked up, the foetus is at risk of stillbirth and neonatal death.”
There might also be long-term consequences such as the risk of neurodevelopmental delay and non-communicable diseases later in life. These include childhood obesity as well as type 2 diabetes, hypertension and strokes in adults.
The UmbiflowTM international study recruited healthy pregnant mothers in five low- and middle-income countries – Ghana, India, Kenya, Rwanda and South Africa – and looked at the percentage of abnormal Dopplers in these countries.
The UmbiBaby study is following up on 91 infants from the South African leg of the international study, assessing them at eight time points over the first two years of life. The PLoS ONE article studied the term-born infants (81) in the first six months of life. The main finding, according to Prof Feucht, was that the growth restriction identified in pregnancy by the UmbiflowTM device continued after birth.
Infants who had an “abnormal Doppler” in utero had a significantly lower fat-free mass (the non-fat portion of the body, which includes bones and muscles). It is also notable that only about a quarter of these infants were small-for-gestational age at birth, which is classified as a birthweight less than that of the 10th percentile.
The assessment of weight at birth would not have identified many of these growth-restricted infants, who may be in need of additional nutritional and neurodevelopment care postpartum. When taking the two definitions together, the growth-restricted infant (as identified by the “abnormal Doppler”) and small-for-gestational age is the most compromised in terms of postnatal growth.
It is therefore recommended that a Doppler device such as the UmbiflowTM, which measures placental function, be utilised routinely during antenatal care, in addition to measuring the infant’s size at birth, as the latter is a once-off measurement that could fail to take into account the infant who might not be small at birth, but who is still at risk of poor growth postnatally.
Click on the infographic in the sidebar to learn more about stillbirths or click the gallery to see how the UmbiflowTM works.
Dr Helen Mulol
April 4, 2022


 Story
Story
University of Pretoria (UP) researchers have found that the antioxidant content of certain types of tea can be likened to that found in recommended portions of fruit and vegetables.
 Infographic
Infographic
Half a cup of black tea, oolong tea or green tea contained the same amount of antioxidants with radical scavenging capabilities (RSC) as that of a 200mg vitamin C tablet.
 Story
Story
Researchers at the University of Pretoria (UP) may have identified the gene that is responsible for diet-related obesity. By exploring the role of the novel gene Slc7a8, they have made a potential breakthrough in current knowledge about the cellular mechanisms that drive fat accumulation. This understanding is crucial in developing effective treatments.
Copyright © University of Pretoria 2025. All rights reserved.


Get Social With Us
Download the UP Mobile App